Best Doctor for Acute Leukemia Treatment in Mumbai, India
What is Acute Leukemia?
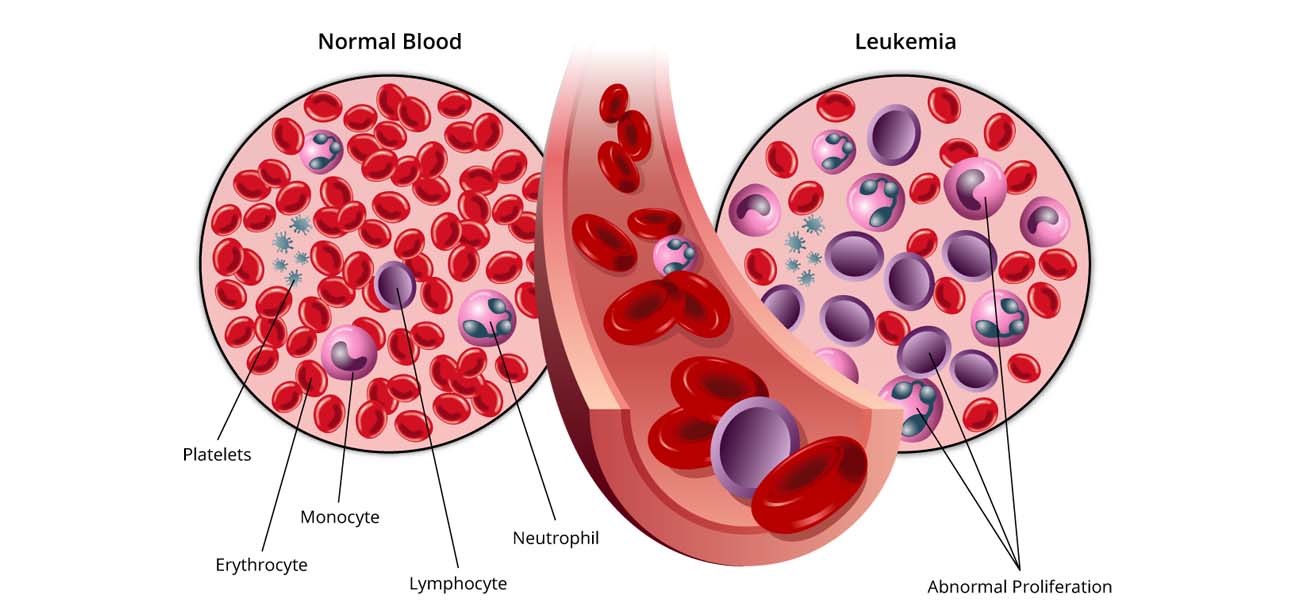
Acute leukemia differs from chronic leukemia in how it develops and worsens. In acute leukemia, the number of abnormal blood cells (blasts) increases much more rapidly than in chronic leukemia. Also, in acute leukemia the blasts remain immature and cannot carry out their normal functions, but in chronic leukemia some of the blasts mature and can function normally.
The two types of acute leukemia are defined by the type of white blood cell that is affected.
Acute lymphocytic leukemia
(ALL) affects lymphoid cells, while acute myelogenous leukemia (AML) affects myeloid cells.
Acute lymphocytic leukemia (ALL), also known as lymphoblastic and lymphoid, is the most common type of leukemia seen in young children. In this type of leukemia, the lymphocytes, the cells that normally fight infection, don’t mature and overproduce. The overproduction of the lymphocytes crowds out the other healthy blood cells. The cause of acute lymphocytic leukemia is unknown; however, it most likely occurs because of a gene mutation and is not inherited.
Acute myelogenous leukemia (AML)
Acute myelogenous leukemia (AML), also known as granulocytic, myelocytic, myeloblastic and myeloid, occurs in both adults and children. In this type of leukemia, the white blood cells called granulocytes don’t mature correctly and the blast cells crowd out the other healthy blood cells. The cause of AML is unknown.
Treatment of Acute Leukemia
Your child’s treatment plan will be determined by a pediatric oncologist and will be based on your child’s age and medical history, the extent of the disease, your child’s tolerance for certain medications and other factors.
Treatment usually begins by addressing some of the symptoms of the leukemia, such as anemia, bleeding and/or infection. In addition, treatment for leukemia may include one or more of the following:
- Chemotherapy
Chemotherapy are medications that helps fight cancer. They are given by mouth, in the vein, in the muscle or under the skin.
- Targeted drug therapy
In recent years, new drugs that target specific parts of cancer cells have been developed. These drugs work differently than standard chemotherapy drugs and often have less severe side effects.
- Radiation therapy
Radiation therapy uses high-energy waves such as x-rays to kill or shrink cancer cells. It is rarely used to treat leukemia in the central nervous system or other places such as the eyes or testes.
- Bone marrow transplant
A bone marrow transplant involves taking cells found in the bone marrow (stem cells), filtering those cells and giving them back to the patient they came from or to another person. The goal of bone marrow transplantation is to replace the diseased, non-functioning bone marrow with healthy bone marrow.
- Blood transfusion
Almost all patients with leukemia require a blood transfusion during their treatment. Blood transfusions use healthy blood cells from donors and help to replace red blood cells, platelets and other blood components. Leukemia often interferes with the production of red blood cells, white blood cells and platelets. A blood transfusion helps to offset this effect of the disease.
- Surgery
Surgery has a very limited role in treating childhood leukemia because leukemia cells spread throughout the bone marrow and to many other organs through the blood. Aside from a possible lymph node biopsy, surgery rarely has any role in the diagnosis or treatment of acute leukemia.
There are various treatment stages in the treatment of acute leukemia.
- Induction therapy
A combination of chemotherapy and/or radiation therapy and medications given to stop the process of abnormal cells being made in the bone marrow. Remission is the goal in this stage of treatment. Remission means the leukemia cells are no longer being made. This phase may last approximately one month and can be repeated if the goal is not achieved.
- Intensification/Consolidation therapy
Continued treatment even though leukemia cells may not be visible. The leukemia cells may not be visible in a blood test or bone marrow examination, but it is possible that the cells are still present in the body.
- Maintenance therapy
This stage maintains leukemia-free bone marrow by continuing less intense chemotherapy for a longer duration. This phase is used for acute lymphocytic leukemia but not for acute myelogenous leukemia. It can last months to several years. Regular visits to your child’s physician are required in order to determine response to treatment, detect any recurrent disease and manage any side effects of the treatment.
Schedule Your Consultation Now
Dr. Shweta Bansal, hematologist-oncologist excels in Acute Leukemia Treatment in Mumbai, offering personalized care and therapies for optimal patient outcomes.
Pediatric Hematology
Copyright © Childhood Cancer Care | Dr. Shweta Bansal.